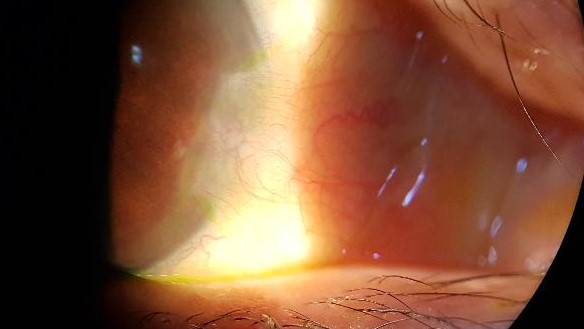

Image above shown , a whitish-looking graft is seen in the scleral bed one day after surgery.
Pterygium is one of the most frequent pathologies of the ocular surface. In fact it is one of the most common cases that we deal with in our daily consultation.
It is a fibrous tissue that grows in the cornea of the eye and that is seen from the outside as a pink area, and that usually affects the innermost part of the eye (near the tear), although it can also appear in the external or temporal area.
Over time, a growth of this tissue occurs and advances towards the cornea, which in turn, pulls from the cornea to go towards the visual axis, if it is not removed by surgery.
The cause is unclear, but as a trigger we will say that it greatly influences the performance of outdoor activities and sports as well as exposure to ultraviolet radiation. Likewise, the dry eye favors it and the circumstances in which the eyes are affected by working in environments with smoke, wind or dust.
It is common to find this pathology in different people due to their professions or hobbies; bricklayers, gardeners, golf players, surfers and people who practice water sports.
There is a hereditary component that occurs more frequently in people with skin pigmentation. In ethnic races, it is common for the healing of their wounds to be more aggressive, which can sometimes occur the appearance of pterygium
The symptomatology of Pterygium has a variety of symptoms, being frequent: dry eyes, discomfort with light or photophobia; eye irritation; feeling of having something inside the eye or even punctures. In more advanced stages, there may be increased astigmatism and blindness if it reaches the visual axis.
The traditional surgery consisted of its excision and removal of the portion of tissue that invaded the cornea. The most distal part of the conjunctiva was removed, the scleral and Tenon beds (underlying layer of the conjunctiva) were cleaned. And after a good cauterization of the bleeding points, the suture was absorbed with resorbable sutures of the two edges of the wound.
But with this technique, widely used throughout the world, the recurrence rate was high, since in many cases the pathological tissue grew even more aggressively.
A few years ago, a modification of the same began, so that exactly the cleaved area of pterygium was measured and carved in part of the healthy conjunctiva of the eye, a graft with the same shape. Through a biological tissue adhesive based on thrombin and fibrinogen, this graft can be attached to the scleral bed of the pterygium without sutures, having many advantages over the classical technique:
1.- Being more laborious, healthy tissue is interposed that greatly decreases the recurrence of abnormal tissue.
2.-The postoperative period is faster since suture removal is not necessary, and there is also a lower risk of traction and opening of the wound edges.
3.- The postoperative pain is less, since except for the first two days in which the corneal ulcer caused by the surgery heals, there are no sutures that rub with the flickering and allows a premature labor incorporation.
Dra. Gloria Carretero León……Eyelid and Ophthalmic Surgery.
Marbella,Estepona, San Pedro
Recent Comments