Lacrimation or “epiphora” is a common case in our clinical practice. Many patients complain that their eyes are always wet and tearing. This causes irritative eczema on the lower eyelids and makes it difficult for them to perform daily activities such as reading.
We must rule out possible causes that produce it, and are as follows:
- Inflammation of the ocular surface, it is treated with anti-inflammatory and artificial tears.
2.- Laxity of the lower eyelid (especially due to age), its treatment is shortening surgery and retension of the cartilaginous portion of the lower eyelid. This is anchored to the periosteum or covering tissue of the outer orbital wall (technique of the tarsal strip or tarsal strip), achieving a substantial improvement in the symptomatology.
3.-Obstructions of the lacrimal ways, the treatment is surgery by an ophthalmologist specializing in oculoplasty.
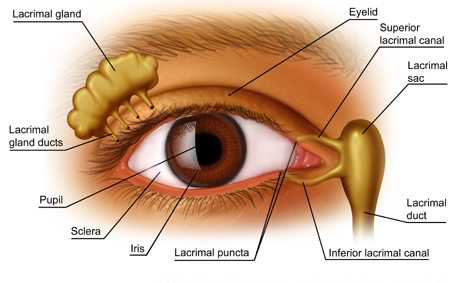
The lacrimal via, is the path of a tear after having been produced by the lacrimal gland and being driven by the flicker towards the orifice lacrimal, and from there it goes to the nose and the oropharynx.
When the tear duct is blocked, this tear can not circulate causing constant tearing and infections in the lacrimal sac (acute dacryocystitis) or conjunctiva (conjunctivitis).
The distal zone is where obstruction is found in 90% of the cases, and there are three types of treatments:
1 – Laser-assisted Dacryocystorhinostomy. A small opening is made in the bone and mucosa with a 200 micron fiber. Doing this, the tear recirculates through the alternative opening towards the nose. There are places where it has stopped performing since it is the least successful and it is very frequent to close again.
2 – Endoscopic dacryocystorhinostomy. It opens a greater communication than using the laser and the help of an otolaryngologist is frequent.
3 – Dacryocystorhinostomy externally. It is the technique with the greatest number of successes and is performed by ophthalmologists who specialize in Oculoplasty. This technique opens a wider communication, performing an osteotomy in the lacrimal crest, a flap is made in the lacrimal sac and another in the nasal mucosa, thus joining both with internal sutures ensuring greater communication.
When the surgery is finished, the lacrimal via is intubated with a silicone implant and tied to the nose and removed after three months. The result of successes with respect to failures is approximately 90% -10%.
Recent Comments