About two decades ago, surgery for myopia and astigmatism with excimer laser, was classically the only existing possibility, this being the technique applied in the operating room for all patients although its graduation was high or low.
This technique is known as LASIK or laser-assisted in situ keratomileusis. It is still current and is the most used technique, with great results and safety. It consists of lifting a corneal flap with microkeratome or femtosecond laser, and ablating the remaining cornea with Excimer laser. The Relex smile technique is a variant technique, in which the complete cut is not produced in 360 degrees, but it is performed intrastromal, with similar effect. The mechanism of action is the evaporation of tissues, causing a corneal flattening and thinning of the cornea to a greater number of corneal microns should be eliminated, producing a very important change in the corneal biomechanics.
After the first few years, it was concluded that a sufficient cornea remnant had to be left, this was to no major abnormalities develop over time as the dreaded Corneal ectasia. What is a corneal deformity that causes irregular astigmatism and decreased visual acuity, and it happens because the corneal architecture is too weak, being this unstable in time.
The number of patients with high myopia for this technique was decreasing little by little since, one of the tests carried out, is knowing the corneal thickness of each candidate, and if it does not exceed the appropriate minimum, it is contraindicated.
That is way, a new technique appeared for them. Today it is performed in some patients from 6 Diopters of myopia.
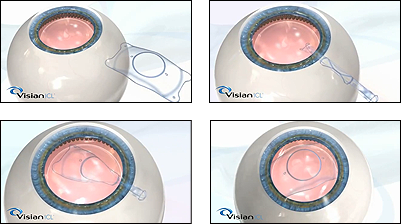
They are pre-crystalline intraocular lenses called ICL, and are implanted to reduce corneal thickness, and thus avoid the aforementioned complications.
Having a large space in the anterior chamber of the eye is necessary, and / or not, having enough corneal thickness for the LASIK technique. It is a procedure performed with topical anesthesia, and it is never done bilaterally.
Always make an eye first, and the next week the second, to check the correct position of the lens inside the eyeball.
It has the advantage of reversibility and visual quality achieved, not having some of the problems with the night lights that do occur with the laser, and not observing decreased sensitivity to contrast.
It is necessary to control the postoperative ocular pressure, it is very important, although the lenses are prepared with a central hole that favors the passage of aqueous humor, avoiding this complication and slowing to a greater extent the appearance of early cataract, more frequent with the old ICL, which were not perforated in the center.
Recent Comments