We continue with our previous news about eyelid surgery, and we will continue talking about two of the most frequent pathologies at the level of Oculoplasty. These are the Ectropion and the Entropion.
ECTROPION
Ectropion is an eversion of the eyelid or an outward tilt of the eyelid, and the main cause is age. It is usually in the lower eyelid and more frequently in senile patients, there is a laxity of certain muscles, and in this case the Orbicularis muscle (muscle that surrounds the eye and is responsible for closing it), the one that is lax. This implies that the retractor muscles of the lower eyelid are stronger (it is the name of the muscles in charge of pulling down the eyelid), and the compensation of forces originate the ectropion.
All this explains an unsightly aspect and, above all, a lot of associated symptoms such as epiphora or continuous tearing and also chronic conjunctivitis and ocular hyperemia, corneal epithelial lesions and blurred vision.
That is why with this pathology, the edge of the eyelid is detached from the eye. In advanced ectropions, there is a thickening and epithelialization of it, being necessary the use of antibiotic lubricants prior to surgery so that it macerates and be able to reverse it.The ocular surgery that is most frequently performed in senile ectropion is the tarsal or trasalStrip technique. This consists of the isolation of the cartilaginous portion of the eyelid, shortening and fixing it to the periosteum of the internal orbital rim. In this way we shorten the surgery and give strength to the eyelid and it remains anchored to a hard surface, thus recovering its functionality and greatly improving all the previous symptoms. In this way its functionality is recovered and all the previous symptoms are greatly improved.


Before and after Ectropion eye surgery Left eye: It is observed how the lower edge of the eye does not contact the eye before the intervention, but it does contact the eye after the surgery.
ENTROPION
Entropion is a pathology just inverse to Ectropion, that is, the eyelid, and especially the lower eyelid, is inverted inwards.
This pathology is also related to age and, in this case, the eyelid muscle retractors do not have the strength to pull downwards and with each blink the orbicularis muscle contracts and straddles, causing the eyelid edge and eyelashes to turn inward.
Initially, all these symptoms appear sporadically and intermittently, but as the weakness of the retractor muscles increases, it becomes a continuous inversion of the eyelid.
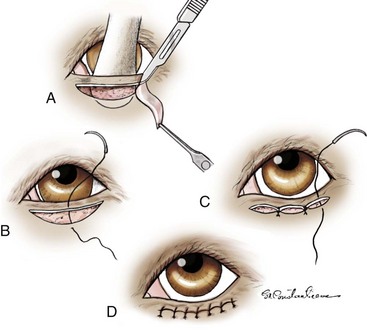
There are many discomforts that this causes to patients, who usually come to the consultation with tape or plasters stuck to the skin of the cheekbone to be able to detach the eyelashes from the eye. In the case of entropion, it is associated with the tarsal strip technique, a reinsertion and fixation to the tarsus of the retractor muscles, which with three sutures of resorbable material are able to shorten them and give them more strength. When the muscles pull down the lower eyelid again, the direction of the lower eyelid is reversed, solving the problem.




These two patients present entropion of the left lower eyelid.
After performing the tarsal strip technique,reattachment of the retractor muscles and shortening of the orbicularis,the edge of the eyelids regains its normal position with respect to the eyeball.
Recent Comments